Basal cell carcinoma (BCC) is a common cutaneous malignancy in Caucasians but has a low incidence in Indian skin. Most commonly, BCC is found in sun-exposed areas, with intermittent ultraviolet exposure as a major risk factor. Although rarely fatal, BCC can cause tissue damage if left untreated. Varicella zoster virus affects both nerve endings and skin, thereby presenting as a rash that may resolve with persisting pain as a symptom. Wolf’s isotopic response (WIR) phenomenon is the formation of a new unrelated disease in the area of a previously healed disease. A 72-year-old housewife with a clinical history of resolved herpes zoster on the scalp presented with an erythematous, atrophic lesion with crusting and fissuring. The post-herpetic neuralgia gradually resolved, but the lesion was not responding to any form of treatment. The histopathological examination demonstrated a picture consistent with superficial basal cell carcinoma. The neurotransmitters released by the nerve endings during an episode of varicella alter the immune control process. This can be a probable cause of a second, unrelated disease, i.e., viral activation in a specific ganglion may alter local immunity, therefore triggering a neoplastic transformation.
| Published in | International Journal of Clinical Dermatology (Volume 8, Issue 2) |
| DOI | 10.11648/j.ijcd.20250802.12 |
| Page(s) | 51-56 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Wolf’s Isotopic Response Phenomenon, Basal Cell Carcinoma, Varicella Zoster
Primary disease | Secondary lesions |
|---|---|
Herpes simplex virus infection [6] | Urticaria |
Herpes zoster virus infection [7, 9, 11, 12] | Chronic GVHD, Acquired perforating folliculitis, Granuloma annulare, acne and comedones, lichen planus, Morphea, linear IgA disease, fungal granuloma, psoriasis, squamous cell carcinoma, basal cell carcinoma, herpetiform pemphigus |
Dermatophytosis [6] | Lichen planus |
Scrofuloderma [6] | Herpes Simplex Virus infection |
Contact dermatitis [9, 13] | Bullous lichen sclerosis et atrophicus, Lichen planus |
Primary disease | Secondary lesions |
|---|---|
Herpes Zoster [10, 11, 13-17] | BCC and Bowenoid papulosis Acute myeloid leukemia |
Vitiligo [18] | BCC |
Nevus sebaceous [19] | BCC |
Hirudiniasis [20] | BCC |
History of trauma (burn, sharp or blunt trauma, varicella scars, vaccination sites) [21-23] | SCC and SCC |
Chronic radiodermatitis [24] | BCC |
BCC | Basal Cell Carcinoma |
UV | Ultraviolet |
HPZ | Herpes Zoster |
PHN | Post-Herpetic Neuralgia |
DEJ | Dermo-Epidermal Junction |
WIR | Wolf’s Isotopic Response |
| [1] | McDaniel B, Badri T, Steele RB. Basal cell carcinoma [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan [updated 2021 Sep 20; cited 2025 Jul 21]. Available from: |
| [2] | Kumar S, Mahajan BB, Kaur S, Yadav A, et al. A study of Basal cell carcinoma in South Asians for risk factor and clinicopathological characterization: A hospital based study. J Skin Cancer. 2014; 2014: 173582. |
| [3] | Bradford PT. Skin cancer in skin of color. Dermatol Nurs. 2009; 21(4): 170-8. |
| [4] | Ruocco V, Ruocco E, Brunetti G, Russo T, Gambardella A, Wolf R. Wolf's post-herpetic isotopic response: Infections, tumors, and immune disorders arising on the site of healed herpetic infection. Clin Dermatol. 2014 Sep-Oct; 32(5): 561-8. |
| [5] | Wolf R, Brenner S, Ruocco V, Filioli FG. Isotopic response. Int J Dermatol. 1995; 34(5): 341-8. |
| [6] | Mahajan R, De D, Saikia U. Wolf's isotopic response: Report of a case and review of literature. Indian J Dermatol. 2014; 59(3): 275-82. |
| [7] | Gupta M. Acneiform eruption at the site of healed herpes zoster: A case of wolf’s isotopic response. Australas J Dermatol. 2016; 57(3): 241. |
| [8] | Earber EM. Psycboneuroimmunology and dermatology. Int J Dermatol. 1993; 32(2): 93-4. |
| [9] | Wang T, Zhang M, Zhang Y, Zhang Y, Zhang S, et al. Wolf’s Isotropic Response after Herpes Zoster Infection: A Study of 24 New Cases and Literature Review. Acta Derm Venereol. 2019; 99(11): 953-9. |
| [10] | Jaka-Moreno A, López-Pestaña A, López-Núñez M, Ormaechea-Pérez N, et al. Wolf's Isotopic Response: A Series of 9 Cases. Actas Dermosifiliogr. 2012; 103(9): 795-805. |
| [11] | Lunge S B, Raichur S R, Wolf's isotopic response of basal cell carcinoma following facial herpes zoster infection: a rare presentation. IP Indian J Clin Exp Dermatol. 2016; 2(2): 64-6. |
| [12] | Tang L, Zhu Y, Wu W. A case report of Wolf’s post-herpetic isotopic response: herpetiform pemphigus. J Inflamm Res. 2025; 18: 4211-6. |
| [13] | Bruin P, McCoy IV WH, Leonardi CL, Martin AG. Wolf’s isotopic response of lichen planus following contact dermatitis. J Am Acad Dermatol. 2022; 27: 128-130. |
| [14] | Kwak JH, Na CH, Kim MS, Choi H. Superficial basal cell carcinoma at the site of herpes zoster: Wolf’s isotopic response or idiopathic? Indian J Dermatol Venereol Leprol. 2024; 91(1): 84-8. |
| [15] | Mishra D, Raji MA. Squamous cell carcinoma occurring at the site of prior herpes zoster of the scalp: Case report of Marjolin ulcer. J Am Geriatr Soc. 2004; 52(7): 1221-2. |
| [16] | Zhu Y, Wu W. Cutaneous myelodysplastic syndrome progressing to acute myeloid leukemia: an unusual presentation of Wolf's isotopic response. An Bras Dermatol. 2024; 99(3): 261-4. |
| [17] | Ruocco E, Cutrì FT, Baroni A. Bowenoid papulosis at the site of herpes progenitalis. Skinmed. 2004; 3(6): 347-9. |
| [18] | Rustemeyer, J.; Günther, L.; Deichert, L. A rare association: Basal cell carcinoma in a vitiliginous macula. Oral Maxillofac. Surg. 2011; 15(3): 175-7. |
| [19] | Dilek N, Bedir R, Yüksel D, Ataseven A. A case of basal cell carcinoma secondary to nevus sebaceous. Int J Case Rep Images. 2014; 5(4): 277-80. |
| [20] | S. Shamsaddini, S. Dabiri. Basal cell carcinoma on nickel dematitis after leech applying. East Mediterr Health J. 2000; 6(1): 197-200. |
| [21] | Noodleman FR, Pollack SV. Trauma as a possible etiologic factor in Basal Cell Carcinoma. J Dermatol Surg Oncol. 1986; 12(8): 841-6. |
| [22] | Keyhani K, Ashenhurst M, Oryschak A. Periocular basal cell carcinoma arising in a site of previous trauma. Can J Ophthalmol. 2007; 42(3): 467-8. |
| [23] | Yoo JJ, Kim HS, Kim JH, Joo M, Kim KJ, Park SJ. Clinical features and treatment outcomes of skin cancer arising from burn scar: A single-institution experience. Tumori. 2014; 100(1): 26-30. |
| [24] | Meibodi NT, Maleki M, Javidi Z, Nahidi Y. Clinicopathological evaluation of radiation induced basal cell carcinoma. Indian J Dermatol. 2008; 53(3): 137-9. |
APA Style
Dhawan, S., Sharma, K. (2025). Wolf’s Isotopic Response in a Post Herpes Zoster Patient Forming Superficial Basal Cell Carcinoma. International Journal of Clinical Dermatology, 8(2), 51-56. https://doi.org/10.11648/j.ijcd.20250802.12
ACS Style
Dhawan, S.; Sharma, K. Wolf’s Isotopic Response in a Post Herpes Zoster Patient Forming Superficial Basal Cell Carcinoma. Int. J. Clin. Dermatol. 2025, 8(2), 51-56. doi: 10.11648/j.ijcd.20250802.12
@article{10.11648/j.ijcd.20250802.12,
author = {Sachin Dhawan and Komal Sharma},
title = {Wolf’s Isotopic Response in a Post Herpes Zoster Patient Forming Superficial Basal Cell Carcinoma
},
journal = {International Journal of Clinical Dermatology},
volume = {8},
number = {2},
pages = {51-56},
doi = {10.11648/j.ijcd.20250802.12},
url = {https://doi.org/10.11648/j.ijcd.20250802.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcd.20250802.12},
abstract = {Basal cell carcinoma (BCC) is a common cutaneous malignancy in Caucasians but has a low incidence in Indian skin. Most commonly, BCC is found in sun-exposed areas, with intermittent ultraviolet exposure as a major risk factor. Although rarely fatal, BCC can cause tissue damage if left untreated. Varicella zoster virus affects both nerve endings and skin, thereby presenting as a rash that may resolve with persisting pain as a symptom. Wolf’s isotopic response (WIR) phenomenon is the formation of a new unrelated disease in the area of a previously healed disease. A 72-year-old housewife with a clinical history of resolved herpes zoster on the scalp presented with an erythematous, atrophic lesion with crusting and fissuring. The post-herpetic neuralgia gradually resolved, but the lesion was not responding to any form of treatment. The histopathological examination demonstrated a picture consistent with superficial basal cell carcinoma. The neurotransmitters released by the nerve endings during an episode of varicella alter the immune control process. This can be a probable cause of a second, unrelated disease, i.e., viral activation in a specific ganglion may alter local immunity, therefore triggering a neoplastic transformation.},
year = {2025}
}
TY - JOUR T1 - Wolf’s Isotopic Response in a Post Herpes Zoster Patient Forming Superficial Basal Cell Carcinoma AU - Sachin Dhawan AU - Komal Sharma Y1 - 2025/08/26 PY - 2025 N1 - https://doi.org/10.11648/j.ijcd.20250802.12 DO - 10.11648/j.ijcd.20250802.12 T2 - International Journal of Clinical Dermatology JF - International Journal of Clinical Dermatology JO - International Journal of Clinical Dermatology SP - 51 EP - 56 PB - Science Publishing Group SN - 2995-1305 UR - https://doi.org/10.11648/j.ijcd.20250802.12 AB - Basal cell carcinoma (BCC) is a common cutaneous malignancy in Caucasians but has a low incidence in Indian skin. Most commonly, BCC is found in sun-exposed areas, with intermittent ultraviolet exposure as a major risk factor. Although rarely fatal, BCC can cause tissue damage if left untreated. Varicella zoster virus affects both nerve endings and skin, thereby presenting as a rash that may resolve with persisting pain as a symptom. Wolf’s isotopic response (WIR) phenomenon is the formation of a new unrelated disease in the area of a previously healed disease. A 72-year-old housewife with a clinical history of resolved herpes zoster on the scalp presented with an erythematous, atrophic lesion with crusting and fissuring. The post-herpetic neuralgia gradually resolved, but the lesion was not responding to any form of treatment. The histopathological examination demonstrated a picture consistent with superficial basal cell carcinoma. The neurotransmitters released by the nerve endings during an episode of varicella alter the immune control process. This can be a probable cause of a second, unrelated disease, i.e., viral activation in a specific ganglion may alter local immunity, therefore triggering a neoplastic transformation. VL - 8 IS - 2 ER -
Derpartment of Dermatology, Aesthetics and Dental Clinic, Gurgaon, India
Department of Dermatology, Healing Hospital, Chandigarh, India

Figure 1. A single lesion on the left side of the scalp with brown crust and associated pain.
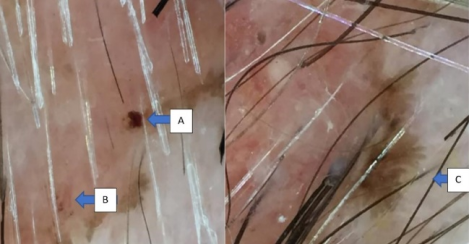
Figure 2. Dermoscopic findings: well-defined grey-brown dots scattered within the lesion (arrow A and arrow B). Leaf-like (Maple leaf-like), bulbous extensions forming the border of the lesion (arrow C). Maple leaf-like areas and brown to blue-grey dots and globules are among the classic BCC-associated dermoscopic features.
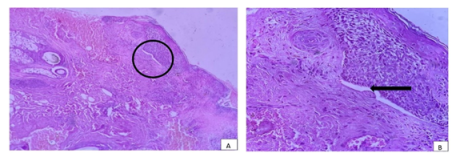
Figure 3. Skin biopsy from the border of the lesion. (A) Haematoxylin and Eosin stain, 40X scanner view. (B) Haematoxylin and Eosin stain, 100X: increased pigment deposits, mitosis, and an increased basaloid cell proliferation with retraction artefact at dermo-epidermal junction (DEJ).
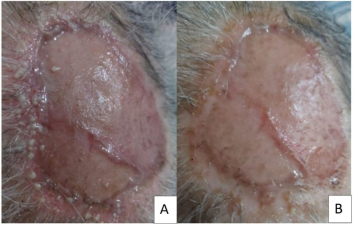
Figure 4. (A) Contact pustulosis due to neomycin ointment on the recipient site. (B) Resolution of contact pustulosis after treatment with 10 days of oral doxycycline.
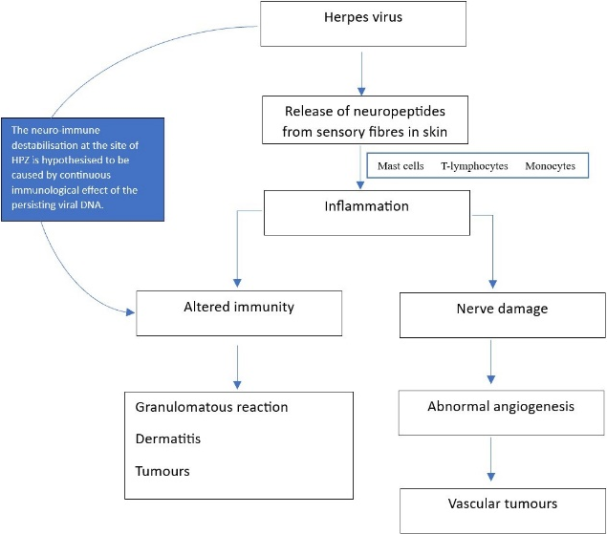
Figure 5. Suggested hypothesis of pathogenesis of Wolf’s Isotopic Response.

